Opioids and Other Psychoactive Substances
Psychoactive substances are chemical compounds that can lead to physical or psychological dependence when consumed repeatedly, often altering brain function and behaviour. Overdose and overuse have caused significant public health concerns due to their potential to cause a wide range of adverse health effects. Addictive substances include alcohol, nicotine, (synthetic) opioids, (natural) opiates, stimulants, and certain sedatives, amongst others.
Primary reference(s)
NIDA 2020 July 6 Drug Misuse and Addiction. Accessed 20 January 2025.
Annotations
Additional scientific description
Opiates are drugs derived from opium, which are alkaloids naturally found in the opium poppy plant Papaver somniferum that upon extraction typically yield (-)-morphine (10-15%), (-)-codeine (3-methylmorphine, 3-4%), and (-)-thebaine (1-2%). On the other hand, the term opioids is used for all substances, either natural or synthetic, that bind to opioid receptors, including the antagonists (NIDA, 2024).
These substances have been consumed as medicine for the treatment of pain but also recreationally for the euphoria and hallucinations that they provoke. The uncontrolled use of these substances (opioid overdose) has resulted in the present so-called "opioid" epidemic responsible for around 80% of the 600,000 deaths reported worldwide in 2019. Common side effects include tolerance and dependence, itching, pupil constriction, constipation, nausea and vomiting, and most importantly, respiratory depression. The major offenders are synthetic opioids other than methadone followed by psychostimulants and finally heroin (WHO, 2023).
Heroin, an acetylated derivative of morphine, was first made in 1874 and later first manufactured in 1898. The acetylation makes the molecule less polar than morphine, so that it crosses the Blood Brain Barrier (BBB) more easily, and once inside the brain, enzymes hydrolyse the esters quite easily resulting in a faster delivery of morphine, which is the actual drug responsible for the observed intense euphoric effects (NIDA, 2011)
Prescription opioids are the leading offenders in drug addiction by several mechanisms such as redirection, over-prescription, or doctor shopping (Skolnick, 2018). Some prescription opioids include hydrocodone bitartrate, oxycodone hydrochloride, oxymorphone hydrochloride, morphine sulfate extended-release and codeine. One of the main contributors has been the oxycodone hrdrochloride pills, where over-prescription of opioids leads to overdoses and addiction.
Other less common and simpler opioids are the morphinans, which are more potent and longer lasting than its morphine counterparts with a higher toxicity. Included in the simpler structures, made by simplification strategies, are the 6,7-benzomorphans (Metazocine/Pentazocine), the 4-phenylpiperidines, and methadone, which is used to treat drug addicts.
One of the opioids of most recent concern, by its potency and overwhelming abuse, is fentanyl and its many analogues. Fentanyl was first synthesized in the early 1960's and is 50-100 times more potent than heroin and 2-3 mg of the opioid can be fatal (Stanley, 2005).
When used under strict medical supervision, fentanyl is safe and appropriate. Fentanyl use mainly relies on treating patients that have become tolerant to opioid therapy for cancer pain and need something stronger. The range of compound amount typically used can be between 50 - 1200 µg (mcg) in different forms of delivery or concentrations. Among the fentanyl approved drugs, we should mention the transdermal patches, sublingual tablets, lollipops, and the injectable forms. The use of fentanyl in colonoscopy studies (25-50 µg) is also common, safe, and significantly shortens recovery times (Stanley, 2005).
Misuse of fentanyl sparked by the illicit market has led to the detection of several forms of the drug, mainly as illegal pills, in different forms and combinations. The ease of synthesing the derivatives coupled with the proliferation of clandestine laboratories with no quality control, has resulted in haphazard combinations of the drug and millions of deaths. Derivatives of considerable importance include furanyl fentanyl, acetylfentanyl, fluorofentanyl (different ring substitutions with the para derivative being more abused), and the extremely potent carfentanil among many others. Carfentanil, by itself, is an animal tranquilizer 100 times more potent than fentanyl and 10,000 times more potent than morphine, and is used in veterinary medicine for the immobilization of large animals such as rhinoceros or elephants. Unfortunately, it has also found its way into street drugs as well. WHO continues to monitor several fentanyl analogues through its surveillance system for new psychoactive substances, alerting countries to the potential dangers associated with these substances (Han, 2019).
More recently, fentanyl and xylazine combinations have been detected in the streets, which has become an emerging threat since July 2023. Xylazine is used in veterinary medicine (mainly with horses) as an anesthetic but its misuse in humans causes euphoric effects, muscle relaxation, and trouble breathing. In addition, users can develop chronic wounds that are difficult to heal and painful. Xylazine is an Alpha-2 agonist, not an opioid, and as such naloxone does not reverse its effects. Presently there is no approved antagonist which can reverse its deleterious effects. Other opioids such as nitazines are also dangerous, as is accidental or deliberate contamination of heroin by fentanyls or nitazenes, which can lead to unexpected toxicity and accidental overdose (Jain 2024).
Alcohol and nicotine are two widely used substances with addictive properties that can have severe consequences for health and well-being. Alcohol is a depressant that enhances the release of dopamine in the brain, creating feelings of relaxation and euphoria. Chronic use can lead to tolerance, dependence, and withdrawal symptoms such as anxiety, tremors, and seizures. Long-term alcohol misuse increases the risk of liver disease, cardiovascular and neurological damage (NIAAA, 2021).
Nicotine, found in tobacco products, is a highly addictive stimulant that rapidly affects the brain, triggering the release of dopamine and reinforcing the habit. Prolonged use of nicotine leads to dependence and withdrawal symptoms like irritability, anxiety, and cravings. It is a major risk factor for respiratory diseases, heart disease, and various cancers, particularly lung cancer. The addictive nature and health risks of both substances underscore the need for effective prevention and support for individuals seeking to overcome their use (Benowitz , 2010).
Metrics and numeric limits
Opioids: Prescription Guidelines
- Morphine Milligram Equivalents (MME): The Centers for Disease Control and Prevention (CDC) recommends avoiding doses of ≥90 MME/day for chronic pain when possible, as higher doses increase the risk of overdose. (CDC, 2022).
- Duration of Use:
- For acute pain, prescriptions should generally not exceed 3-7 days, as longer durations significantly increase the risk of dependency (Dowell, 2016).
- Naloxone Prescription: Co-prescription of naloxone is recommended for patients at higher risk of opioid overdose, such as those on ≥50 MME/day (Dowell, 2016).
Alcohol: Moderate Drinking Guidelines:
- United States Dietary Guidelines (2020-2025):
- Moderate drinking is defined as:
- Up to 1 drink per day for women.
- Up to 2 drinks per day for men.
- One standard drink is: 14 grams of pure alcohol, equivalent to:
- 12 oz of beer (5% alcohol).
- 5 oz of wine (12% alcohol).
- 1.5 oz of distilled spirits (40% alcohol). (U.S. Department of Health and Human Services, 2020).
- Moderate drinking is defined as:
- Weekly Limits:
- The National Institute on Alcohol Abuse and Alcoholism (NIAAA) suggests: No more than 7 drinks per week for average women and 14 drinks per week for average men to reduce risks of alcohol-related harm (NIAAA, 2021). Women who are pregnant or planning a pregnancy should not drink alcohol.
Key relevant UN convention / multilateral treaty
Several key United Nations conventions and multilateral treaties address issues related to the control of addictive substances such as opioids, alcohol, and nicotine. Here's an overview:
Opioids:
Single Convention on Narcotic Drugs (1961, as amended in 1972): Establishes international control over narcotic drugs, including opioids, to limit their use to medical and scientific purposes while preventing illicit production and trafficking. Administered by the International Narcotics Control Board (INCB).
Convention on Psychotropic Substances (1971): Aims to control psychotropic substances, including certain synthetic opioids, to prevent misuse while ensuring their availability for legitimate purposes.
United Nations Convention against Illicit Traffic in Narcotic Drugs and
Alcohol: No specific global treaty regulates alcohol in the same way as narcotics, but alcohol is indirectly addressed under health and public policy frameworks:
Global Strategy to Reduce the Harmful Use of Alcohol (2010): A non-binding framework by the World Health Organization (WHO) encouraging member states to implement policies addressing alcohol misuse.
WHO Framework Convention on Tobacco Control (2003): Although focused on tobacco, this treaty includes measures related to the dual-use of substances like alcohol and tobacco, recognizing the intersection of public health challenges.
Nicotine (Tobacco): WHO Framework Convention on Tobacco Control (FCTC, 2003): The first legally binding health treaty under WHO, focusing on reducing tobacco consumption and exposure to nicotine products. Includes measures on advertising bans, tax policies, and restrictions on public smoking.
Drivers
Hazard Drivers for Opioid Dependence: There are a number of risk factors for opioid overdose as described by WHO (WHO, 2023). These include:
- having an opioid use disorder;
- taking opioids by injection;
- resumption of opioid use after an extended period of abstinence (e.g. following detoxification, release from incarceration, cessation of treatment);
- using prescription opioids without medical supervision;
- high prescribed dosage of opioids (more than 100 mg of morphine or equivalent daily).
- using opioids in combination with alcohol and/or other substances or medicines that suppress respiratory function such as benzodiazepines, barbiturates, anaesthetics or some pain medications; and
- having concurrent medical conditions such as HIV, liver or lung diseases or mental health conditions.
Males, people of older age and people with low socio-economic status are at higher risk of opioid overdose than women, people of young age groups and people with higher socio-economic status.
Hazard Drivers for Alcohol Dependence (Mustafa 2024):
A. Biological and Genetic Factors
- Family History of Addiction: Having a parent or close relative with alcohol addiction increases the risk due to genetic predisposition.
- Neurochemical Imbalances: Altered levels of neurotransmitters, such as dopamine, can make individuals more susceptible to addiction.
- Early Onset of Drinking: Initiating alcohol consumption at a young age is linked to higher risk of developing dependence.
B. Psychological Factors
- Mental Health Disorders: Conditions like depression, anxiety, or PTSD often coexist with alcohol misuse.
- Stress and Coping Mechanisms: Using alcohol as a coping mechanism for stress increases the risk of dependency.
C. Social and Environmental Factors
- Peer Pressure: Strong influence from peers can lead to habitual alcohol use.
- Cultural Norms: Societal attitudes that normalize or glamorize drinking can increase risk.
- Availability and Accessibility: Easy access to alcohol significantly raises the likelihood of abuse.
D. Other Factors
- Trauma and Adverse Childhood Experiences (ACEs): Early-life trauma is strongly associated with addiction risks.
- Lack of Education: Poor understanding of the risks associated with excessive alcohol consumption can contribute.
Hazard Drivers for nicotine dependence (Benowitz 2010):
A. Biological and Genetic Factors
- Genetic Susceptibility: Genetic variations can affect how the body processes nicotine and the likelihood of addiction.
- Adolescent Brain Development: Young brains are particularly sensitive to the effects of nicotine, increasing addiction risks.
B. Psychological Factors
- Coexisting Mental Health Conditions: Anxiety and depressive disorders are common among individuals with nicotine dependence.
- Impulsivity and Sensation-Seeking: Personality traits that favour risky behaviours are linked to higher nicotine use.
C. Social and Environmental Factors
- Peer and Social Influence: Adolescents are particularly vulnerable to smoking due to peer pressure.
- Marketing and Advertising: Targeted advertisements and media representations glamorizing smoking contribute significantly.
- Family Smoking Habits: Exposure to smoking within the household normalizes the behaviour and increases risk
Impacts
Opioids are the deadliest drug type. According to the US Drug Enforcement Administration (DEA) seven out of ten illegal fake pills in the streets with fentanyl contain a potentially lethal dose (at least 2 mg of fentanyl). Drug traffickers are using fake pills to exploit the opioid crisis and prescription drug misuse. In 2022, an estimated 110,757 people died by drug poisoning in the United States. Fentanyl, the synthetic opioid most found in fake pills, is the primary driver in this alarming increase in poisoning deaths. According to WHO estimates, approximately 125,000 people died of opioid overdose in 2019.
Multi-hazard context
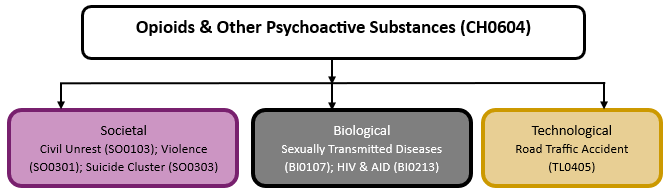
The figure below summarises common interactions between opioids & other addictive substances and other hazards. This information should be used with caution and not be solely relied upon in Disaster Risk Management, particularly as some interactions may not have been included. Note that hazardous events occurring together or locally in space or time may not necessarily cause, amplify or be otherwise related to each other. Specific examples of multi-hazard context can be found in the ‘Hazard drivers’ and ‘Impacts’ sections above.
Multi-hazard diagram
Risk Management
Detection of fentanyl is difficult since it has no taste, no smell, and cannot be distinguished by touch. Some recent detection efforts include fentanyl test strips (FTS) and advanced handheld Raman spectrometers analysers such as Tactic ID or TruNarc™, which are narcotic analysers. Portable mass spectrometers may also prove useful. FTS are small strips of paper that can detect the presence of fentanyl in different kinds of drugs and drug forms and can inform people about the presence of fentanyl so they can take steps to reduce their risk of overdose. There is also a commercial strip version that combines both fentanyl and xylazine in one test strip. The Raman spectrometers allow the first responders to quickly and accurately identify key drugs of abuse anywhere at any time without opening the containers (Crocombe 2023).
Uncontrolled opioid use can lead to dependence, both physical and mental. There are observable withdrawal symptoms and a sustained mental need for the drug or substance. An overdose needs immediate attention due to its fatal consequences. The best is the use of an antidote, now more commonly used is naloxone, which is an antagonist of the opioid receptors and reverses the overdose (van Dorp, 2007). Naloxone comes in different forms, but the most common is the nasal spray with similar action times as an intramuscular injection. Sometimes several doses of are needed to reverse a strong opioid overdose. WHO recommends that naloxone be made available to people likely to witness an opioid overdose, as well as training in the management of opioid overdose. More recently, in the US, a similar delivery method has been manufactured with nalmefene with the advantage of having a longer half-life (11.4 hrs) vs. 1.2 hrs than naloxone (Green 2024).
WHO recommends the use of a range of treatment options for opioid dependence. These include opioid agonist maintenance treatment (with medicines such as methadone and buprenorphine), which has the strongest evidence of effectiveness and cost-effectiveness, as well as psychosocial treatment and support, and pharmacological treatment with opioid antagonists (such as naltrexone).
Monitoring
No Information Available
References
Alpert, A. et al., 2022. ORIGINS OF THE OPIOID CRISIS AND ITS ENDURING IMPACTS - PubMed Q J Econ. 2022 May;137(2):1139-1179. doi: 10.1093/qje/qjab043 Accessed 21 April 2025
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
Benowitz, N. L., 2010. Nicotine addiction. The New England Journal of Medicine, 362(24), 2295–2303. doi:10.1056/NEJMra080989
Centers for Disease Control and Prevention, 2020. Health effects of cigarette smoking. Retrieved from https://www.cdc.gov Accessed 20 January 2025.
CDC, 2020 Emergency Preparedness and Response: Increase in Fatal Drug Overdoses Across the United States Driven by Synthetic Opioids Before and During the COVID-19 Pandemic, 17 December 2020. Accessed 20 January 2025.
CDC, 2022. CDC Clinical Practice Guideline for Prescribing Opioids for Pain — United States, 2022, Recommendations and Reports / November 4, 2022 / 71(3);1–95 CDC Clinical Practice Guideline for Prescribing Opioids for Pain — United States, 2022 | MMWR, Accessed 20 January 2025
Crocombe, R.A. et al., 2023. Field-portable detection of fentanyl and its analogs: A review. J Forensic Sci. 2023 Sep;68(5):1570-1600. doi: 10.1111/1556-4029.15355.
Dowell, D., et al., 2016. CDC Guidelines for Prescribing Opioids for Chronic Pain. JAMA, 315(15), 1624–1645. CDC Guideline for Prescribing Opioids for Chronic Pain—Udnited States, 2016 | Pain Medicine | JAMA | JAMA Network Accessed 20 January 2025
Foglia, R. , 2021. Curr Addict Rep. 2021;8(2):319-329. doi: 10.1007/s40429-021-00368-6.
Green, M. et al., 2024. Nalmefene Hydrochloride: Potential Implications for Treating Alcohol and Opioid Use Disorder. Subst Abuse Rehabil. 2024 Apr 3;15:43-57. doi: 10.2147/SAR.S431270.
Han, Y. et al., 2019. Transl Psychiatry. 2019 Nov 11;9(1):282. doi: 10.1038/s41398-019-0625-0. Accessed 21 April 2025
Jain, L. et al., 2024. World J Psychiatry. 2024 Jun 19;14(6):760-766. doi: 10.5498/wjp.v14.i6.760.
Moustafa, A.A. et al., 2024. Drinking motives as a predictor of readiness to change alcohol use. Curr Psychol 43, 1264–1277 (2024). https://doi.org/10.1007/s12144-023-04245-5 Accessed 21 April 2025
NIAAA, 2021 National Institute on Alcohol Abuse and Alcoholism. (2021). Alcohol’s effects on the body. Retrieved from . Accessed 20 January 2025.
NIAAA, 2021. Drinking Levels Defined. Understanding Alcohol Drinking Patterns | National Institute on Alcohol Abuse and Alcoholism (NIAAA) accessed 20 January 2025
NIDA, 2011. Heroin Research Report: Overview | NIDA Accessed 21 April 2025
NIDA, 2024. Opioids | National Institute on Drug Abuse (NIDA) Accessed 21 April 2025
Rehm, J., et al. (2009). Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. The Lancet, 373(9682), 2223–2233. doi:10.1016/S0140-6736(09)60746-7
Skolnick, P., 2018. The Opioid Epidemic: Crisis and Solutions - PubMed Annu Rev Pharmacol Toxicol. 2018 Jan 6:58:143-159 Accessed 21 April 2025
Stanley, T.H., 2005. J Pain Symptom Manage 2005 May;29(5 Suppl):S67-71. doi: 10.1016/j.jpainsymman.2005.01.009
Trends and Geographic Patterns and Synthetic Opioid Overdose Deaths – United States, 2013-2019. Morbidity and Mortality Weekly Report, Vol. 70, No 6. Available at: https://www.cdc.gov/mmwr/volumes/70/wr/mm7006a4.htm?s_cid=mm7006a4_w Accessed 20 January 2025.
United Nations Office on Drugs and Crime (UNODC), 1961. Single Convention on Narcotic Drugs, 1961. Retrieved from https://www.unodc.org/unodc/en/treaties/single-convention.html Accessed 20 January 2025.
United Nations Office on Drugs and Crime (UNODC), 1971. Convention on Psychotropic Substances. Retrieved from https://www.unodc.org/unodc/en/treaties/psychotropics.html Accessed 20 January 2025.
United Nations Office on Drugs and Crime (UNODC),1988. Convention against Illicit Traffic in Narcotic Drugs and Psychotropic Substances. Retrieved from https://www.unodc.org/unodc/en/treaties/illicit-trafficking.html Accessed 20 January 2025.
UNODC, 2023. World Drug Report 2023. Available at: https://www.unodc.org/unodc/en/data-and-analysis/world-drug-report-2023.html Accessed 20 January 2025.
UNODC-WHO Stop-Overdose-Safely (S-O-S) project implementation in Kazakhstan, Kyrgyzstan, Tajikistan and Ukraine: summary report. WHO and UNODC, 2021. Available at: https://apps.who.int/iris/handle/10665/340497 Accessed 20 January 2025.
U.S. Department of Health and Human Services, 2014. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: Centers for Disease Control and Prevention. Accessed 20 January 2025.
U.S. Department of Health and Human Services, 2020. Dietary Guidelines for Americans. Dietary Guidelines for Americans, 2020-2025 accessed 20 January 2025
van Dorp, E., et al., 2007. Naloxone treatment in opioid addiction: the risks and benefits. Expert Opin Drug Saf. 2007 Mar;6(2):125-32. doi: 10.1517/14740338.6.2.125.
World Health Organization (WHO), 2003. WHO Framework Convention on Tobacco Control. Retrieved from https://fctc.who.int/ Accessed 20 January 2025.
World Health Organization (WHO), 2010. Global Strategy to Reduce the Harmful Use of Alcohol. Retrieved from https://www.who.int/publications-detail/global-strategy-to-reduce-the-harmful-use-of-alcohol Accessed 20 January 2025.
World Health Organization (WHO), 2019. International Classification of Diseases for Mortality and Morbidity Statistics. Eleventh Revision. Accessed 20 January 2025.
WHO Expert Committee on Drug Dependence: forty-third report (WHO Technical Report Series, No. 1034). WHO, 2021. Available at: https://www.who.int/publications/i/item/9789240023024 Accessed 20 January 2025.
World Health Organization (WHO), 2023. https://www.who.int/news-room/fact-sheets/detail/opioid-overdose Accessed 21 April 2025