Antimicrobial Resistance
Antimicrobial-resistant (AMR) microorganisms are bacteria, fungi, viruses, or parasites that evolve to withstand antimicrobial treatments, including antibiotics, antifungals, antivirals, and antiparasitics. These resistant microorganisms, make infections harder to treat, increasing the risk of disease spread, severe illness, and mortality. AMR is a major global public health and food security challenge and is driven by the misuse and overuse of antimicrobials in human medicine, animal health, and plant production and protection, as well as environmental contamination (adapted from WHO, 2023 and FAO, 2025).
Primary reference(s)
WHO, 2023. Antimicrobial resistance. World Health Organization (WHO). Accessed 27 May 2025.
FAO, 2025. Antimicrobial resistance. Food and Agriculture Organization (FAO). Accessed 27 May 2025.
Annotations
Additional scientific description
Antimicrobial resistance (AMR) is a natural process that happens over time through genetic changes in pathogens. Its emergence and spread is accelerated by human activity, mainly the misuse and overuse of antimicrobials to treat, prevent or control infections in humans, animals and plants (WHO, 2023).
Antimicrobial medicines are the cornerstone of modern medicine. The emergence and spread of drug-resistant pathogens threatens our ability to treat common infections and to perform life-saving procedures including cancer chemotherapy and caesarean section, hip replacements, organ transplantation and other surgeries. In addition, drug-resistant infections impact the health of animals and plants, reduce productivity in farms, and threaten food security. AMR has significant costs for both health systems and national economies overall. For example, it creates the need for more expensive and intensive care, affects the productivity of patients or their caregivers through prolonged hospital stays, and harms agricultural productivity (WHO, 2023).
AMR is a problem for all countries at all income levels. Its spread does not recognize country borders. Contributing factors include lack of access to clean water, sanitation and hygiene (WASH) for both humans and animals; poor infection and disease prevention and control in homes, healthcare facilities and farms; poor access to quality and affordable vaccines, diagnostics and medicines; lack of awareness and knowledge; and lack of enforcement of relevant legislation. People living in low-resource settings and vulnerable populations are especially impacted by both the drivers and consequences of AMR (WHO, 2023).
The economic losses due to AMR in agrifood systems could exceed USD100 trillion by 2050 due to reduced productivity, trade restrictions, and increased healthcare costs (Baudoin et al., 2021).
Examples of AMR in HIV, tuberculosis and malaria are summarised below:
- Over the past decade, the world has witnessed an unprecedented increase in the use of antiretroviral therapy (ART), which has saved the lives of tens of millions of people living with HIV/AIDS. At the end of 2021, 28.7 million people, out of an estimated 38.4 million people living with HIV, were receiving ART globally. Increased use of HIV medicines has been accompanied by the emergence of HIV drug resistance - the levels of which have steadily increased in recent years. HIV drug resistance is caused by changes in the genetic structure of HIV that affect the ability of drugs to block the replication of the virus. All current antiretroviral drugs, including newer classes, are at risk of becoming partly or fully inactive due to the emergence of drug-resistant virus strains (WHO, no date a).
- Multidrug-resistant TB (MDR-TB) is a form of TB disease caused by a strain of M. tuberculosis complex that is resistant to rifampicin and isoniazid. Globally, an estimated 410 000 people (95% UI: 370,000-450,000) developed multidrug- or rifampicin-resistant tuberculosis (MDR/RR-TB) in 2022. The treatment success rate for people diagnosed with MDR/RR-TB has steadily improved, but it remains alarmingly low. Globally, in 2020, the treatment success rate was 63%, up from 60% in 2019 and 50% in 2012 (WHO, 2024).
- The development of resistance to drugs poses one of the greatest threats to malaria control and results in increased malaria morbidity and mortality. Resistance to currently available antimalarial drugs has been confirmed in only two of the four human malaria parasite species, Plasmodium falciparum and P. vivax (CDC, 2024).
AMR is a complex problem that affects all of society and is driven by many interconnected factors. Single, isolated interventions have limited impact. Coordinated action is required to minimize the emergence and spread of antimicrobial resistance. All countries need national action plans on AMR to address the issue comprehensively. Greater innovation and investment are required in the research and development of new antimicrobial medicines, vaccines, and diagnostic tools (WHO, 2023).
Metrics and numeric limits
AMR is a growing global health crisis requiring multisectoral collaboration and sharing of information across multiple sectors, including a series of publications on metrics:
- In 2016, O'Neil and colleagues reported that their estimates project that, without effective intervention, AMR could result in 10 million deaths annually by 2050, surpassing mortality rates of major diseases such as cancer (O'Neil, 2016).
- Murray et al. (2022) estimated that bacterial AMR was directly responsible for 1.27 million deaths in 2019 and is associated with 4.95 million deaths globally, with the highest burden in low- and middle-income countries (Murray et al., 2022).
- Naghavi et al. (2024) reported, in their systematic analysis, that AMR-related mortality will continue to rise, with estimates of 1.91 million deaths directly attributable to AMR and 8.22 million associated deaths projected for 2050. The most affected regions will be South Asia, Latin America, and Sub-Saharan Africa, with the largest increase in AMR-related deaths occurring among individuals over 70 years old (Naghavi et al., 2024).
- Lewnard et al. (2024) reported that examining the AMR burden in low- and middle-income countries (LMICs) found that improving infection prevention and control (IPC) programs in LMIC healthcare settings could prevent at least 337,000 AMR-associated deaths annually (Lewnard et al., 2024).
The Food and Agriculture Organization of the United Nations (FAO) and WHO have published maximum residue limits in food products (FAO & WHO, 2018b, c).
Note: Antibiotic resistance has a narrower definition referring only to resistance to antibiotics which target bacteria while antimicrobial resistance relates to resistance or a broader range of microbes (bacteria, viruses, fungi, protozoa) and to a broader range of agents (antibiotics, antivirals, antifungals, antiprotozoals) (WHO, 2023).
Key relevant UN convention / multilateral treaty
The United Nations General Assembly adopted a Political Declaration on Antimicrobial Resistance during its seventy-ninth session on 7 October 2024. The full text of the declaration is available in the official UN document A/79/L.5.
WHO Global Action Plan on AMR. 2015 (WHO, 2015).
FAO Action Plan on Antimicrobial Resistance 2021–2025 (FAO, 2025).
Foodborne antimicrobial resistance – Compendium of Codex standards. (FAO & WHO. 2023).
Memorandum of Understanding regarding cooperation to combat health risks at the animal-human-ecosystem interface in the context of the One Health approach and including antimicrobial resistance. (FAO, WOAH, WHO, UNEP, 2022).
International Health Regulations (2005), 3rd ed. (WHO, 2016).
Drivers
Excessive and inappropriate use of antimicrobial agents in a range of sectors (human health, animal health, crop production), together with other aspects, such as lack of proper waste management or appropriate waste treatment, are key drivers in the exacerbation of antimicrobial resistance. Much attention has been focused on human exposure to antimicrobial-resistant pathogens in hospitals and similar settings and the implications for public health (FAO & WHO, 2018a).
The availability and use of antimicrobial drugs for human health as well as in terrestrial and aquatic animals and in crop production is essential to both health and productivity. Development and transmission of antimicrobial resistance through the food chain is complex with multiple contributing factors, hence addressing it using a coordinated, 'one health' response provides the most effective approach (FAO & WHO, 2018a).
The increase in antimicrobial resistance is a major global threat of increasing concern to human, animal and plant health. It also has implications for both food safety and food security and the economic wellbeing of millions of farming households (FAO & WHO, 2018a).
Ensuring universal access to high-quality water, sanitation, and hygiene (WASH) services could prevent 247,800 AMR-related deaths, while expanded vaccination programs could prevent 181,500 deaths by reducing both resistant infections and antibiotic consumption (Lewnard et al., 2024).
Impacts
Antimicrobial resistance (AMR) is one of the top global public health and development threats. It is estimated that bacterial AMR was directly responsible for 1.27 million global deaths in 2019 and contributed to 4.95 million deaths (WHO, 2023). Other impacts include:
- The misuse and overuse of antimicrobials in humans, animals and plants are the main drivers in the development of drug-resistant pathogens (WHO, 2023).
- AMR affects countries in all regions and at all income levels. Its drivers and consequences are exacerbated by poverty and inequality, and low- and middle-income countries are most affected (WHO, 2023).
- AMR puts many of the gains of modern medicine at risk. It makes infections harder to treat and makes other medical procedures and treatments – such as surgery, caesarean sections and cancer chemotherapy – much riskier (WHO, 2023).
- The world faces an antibiotics pipeline and access crisis. There is an inadequate research and development pipeline in the face of rising levels of resistance, and an urgent need for additional measures to ensure equitable access to new and existing vaccines, diagnostics and medicines (WHO, 2023).
- In addition to death and disability, AMR has significant economic costs. The World Bank estimates that AMR could result in US$ 1 trillion in additional healthcare costs by 2050, and US$ 1 trillion to US$ 3.4 trillion in gross domestic product (GDP) losses per year by 2030 (WHO, 2023).
- Priorities to address AMR in human health include preventing all infections, which may result in inappropriate use of antimicrobials; ensuring universal access to quality diagnosis and appropriate treatment of infections; and strategic information and innovation, for example, surveillance of AMR and antimicrobial consumption/use, and research and development for novel vaccines, diagnostics and medicines (WHO, 2023).
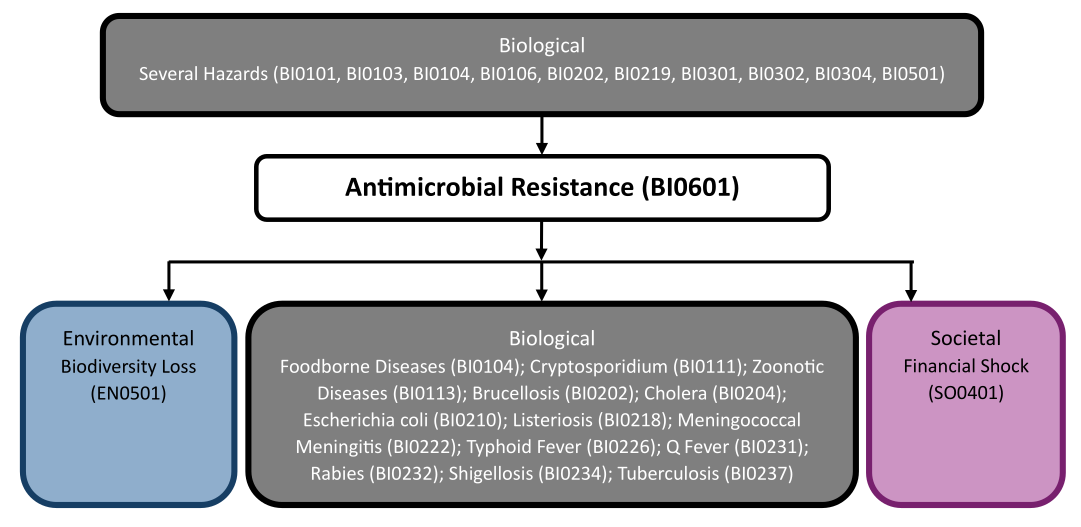
Multi-hazard context
The figure below summarises common interactions between antimicrobial resistance and other hazards. This information should be used with caution and not be solely relied upon in Disaster Risk Management, particularly as some interactions may not have been included. Note that hazardous events occurring together or locally in space or time may not necessarily cause, amplify, or be otherwise related to each other. Specific examples of multi-hazard context can be found in the ‘Hazard drivers’ and ‘Impacts’ sections above.
Multi-hazard diagram
Risk Management
The Quadripartite consisting of the World Health Organization (WHO), the Food and Agriculture Organization of the United Nations (FAO), the World Organization for Animal Health (WOAH), and the United Nations Environment Programme (UNEP) collaborate through a ‘One Health’ approach to promote good practices to prevent and mitigate the emergence and spread of AMR through complementary strategies which include:
- One Health approach: AMR is a complex problem that requires sector-specific actions in the human health, food production, animal and environmental sectors, and a coordinated approach across these sectors. One Health refers to an integrated, unifying approach that aims to achieve optimal and sustainable health outcomes for people, animals and ecosystems. It recognizes that the health of humans, domestic and wild animals, plants and the wider environment are closely linked and interdependent. The One Health approach to preventing and controlling AMR brings together stakeholders from relevant sectors to communicate and work together in the design, implementation and monitoring of programmes, policies, legislation and research to mitigate AMR and attain better health and economic outcomes (WHO, no date a).
- Global Action Plan on Antimicrobial Resistance (GAP-AMR) addresses AMR globally and was adopted in 2015 by the World Health Assembly, emphasizing five strategic objectives: improving awareness and understanding of AMR, strengthening knowledge through surveillance and research, reducing the incidence of infection, optimizing the use of antimicrobial agents, and developing the economic case for sustainable investment. A political declaration endorsed by Heads of State at the United Nations General Assembly in New York in September 2016 reinforced global commitment to addressing AMR through coordinated multisectoral actions across human health, animal health, plant health, and the environment (UNGA, 2024). This commitment was further strengthened by the 2024 Political Declaration on AMR, which emphasized the urgent need for accelerated actions, increased investments, and stronger international collaboration to mitigate AMR's impact on global health, food security, and sustainable development (UNGA, 2024).
- Quadripartite Joint Secretariat on Antimicrobial Resistance: To coordinate the One Health global response to AMR, WHO works closely with the Food and Agriculture Organization of the United Nations (FAO), the UN Environment Programme (UNEP) and the World Organisation for Animal Health (WOAH). The 4 organizations (FAO, UNEP, WHO and WOAH) are known as the Quadripartite Organizations. A quadripartite joint secretariat is hosted by WHO to drive multi-stakeholder engagement in AMR. This has supported the establishment of the Global Leaders Group on AMR, which began its work in November 2020, and the Multi-Stakeholder Partnership Platform, which was launched in November 2022, and several technical working groups (FAO, WOAH, WHO, UNEP, 2022).
As a Quadripartite, WHO, FAO, WOAH, and UNEP jointly implement initiatives such as the AMR Multi-Partner Trust Fund, which mobilizes resources to support national AMR action plans, and the One Health Joint Plan of Action, which fosters cross-sectoral coordination. Additionally, global governance mechanisms like the Global Leaders Group on AMR ensure policy coherence and stakeholder engagement at all levels. Each quadripartite organisation contributes as follows:
- WHO leads multiple initiatives to combat AMR, prioritizing improved antimicrobial stewardship programs and enhancing monitoring and surveillance of AMR and antimicrobial use (AMU) in humans through the Global Antimicrobial Resistance Surveillance System (GLASS) (WHO, no date b), The organization also fosters research and development of new antimicrobial treatments through the Global Antibiotic Research and Development Partnership (GARDP) (WHO, no date c).
- FAO is strongly focused on capacity building for good practices, prudent antimicrobial use, strengthening regulatory frameworks and developing robust AMR and AMU surveillance systems in food and agriculture through the recently launched the “Reduce the Need of Antimicrobials in Farms” (RENOFARM) initiative for sustainable livestock transformation (FAO, no date a)., and the International FAO AMR Monitoring (InFARM) system (FAO, no date b) It has also developed capacity building tools such as the FAO Assessment Tool for Laboratories and AMR Surveillance Systems (FAO-ATLASS) to improve laboratory capacities worldwide (FAO, no date c), FAO supports the implementation of good practices in livestock, aquaculture, and plant production and protection to mitigate AMR risks (FAO, 2021).
- WOAH contributes by strengthening AMU data collection and monitoring in animal health through the WOAH ANIMUSE database (WOAH, no date). It also supports national veterinary legislation and capacity-building for prudent antimicrobial use in veterinary medicine.
- UNEP plays a key role in addressing the environmental dimensions of AMR, conducting research on AMR contamination in water, soil, and waste management, and strengthening policies to reduce AMR pollutants from pharmaceuticals and agricultural runoff (UNEP, no date).
Monitoring
The section and the table below offer an overview of monitoring for antimicrobial resistance. This information can be used for forecasting within a national early warning system (EWS). Since EWS capacities and processes differ across countries, the most current and specific information regarding EWS should be obtained from the appropriate national or regional agency/authority responsible for disaster management.
| Which institution(s) produce(s) Disaster Risk Data/Information? |
|
| How is the Hazard Observed/Monitored/Forecast? | Global and national surveillance systems that track AMR (and AMU) in humans, animals, food, and the environment using laboratory-based testing, genomic sequencing, epidemiological studies, and risk modelling to detect trends, assess risks, and predict future resistance patterns. |
AMR early warning systems have lead times ranging from months to years, depending on the surveillance approach. Laboratory-based monitoring (phenotypic and genomic testing) can detect emerging resistance within weeks to months, while AMR epidemiological modelling and AMU trend analysis help forecast resistance spread over months to years. Environmental and One Health surveillance provide early indicators of resistance evolution, but their lead times depend on data integration and sampling frequency. Unlike acute disease outbreaks, AMR trends develop gradually, requiring continuous monitoring to enable timely policy and stewardship interventions (Ho et al, 2025).
References
Baudoin, F., Hogeveen, H., Wauters, E., 2021. Reducing Antimicrobial Use and Dependence in Livestock Production Systems: A Social and Economic Sciences Perspective on an Interdisciplinary Approach. Front Vet Sci. 18;8:584593. doi: 10.3389/fvets.2021.584593. PMID: 33816582; PMCID: PMC8012488. Accessed 28 May 2025.
CDC, 2024. Drug Resistance in the Malaria-Endemic World, Centers for Disease Control and Prevention (CDC). Accessed 28 May 2025.
FAO, 2021. The FAO Action Plan on Antimicrobial Resistance 2021–2025. Food and Agriculture Organization of the United Nations (FAO). Accessed 19 April 2025.
FAO, 2025. Antimicrobial resistance. Food and Agriculture Organization (FAO). Accessed 27 May 2025.
FAO, no date a. Reduce the Need for Antimicrobials on Farms for Sustainable Agrifood Systems Transformation – Antimicrobial Resistance. Food and Agriculture Organization of the United Nations (FAO). Accessed 28 May 2025.
FAO, no date b. InFARM System - Generating science-based evidence in food and agriculture sectors to tackle AMR. Food and Agriculture Organization of the United Nations (FAO). Accessed 19 April 2025.
FAO, no date c. FAO Assessment Tool for Laboratories and AMR Surveillance Systems (FAO-ATLASS). Food and Agriculture Organization of the United Nations (FAO). Accessed 19 April 2025.
FAO, WHO, 2023. Foodborne antimicrobial resistance – Compendium of Codex standards. First revision. Codex Alimentarius Commission. Rome. Food and Agriculture Organization of the United Nations (FAO) and World Health Organization (WHO). DOI: 10.4060/cb8554e. Accessed 19 April 2025.
FAO, WOAH, WHO, UNEP, 2022. Memorandum of Understanding regarding cooperation to combat health risks at the animal-human-ecosystem interface in the context of the One Health approach and including antimicrobial resistance. Food and Agriculture Organization of the United Nations (FAO), the United Nations Environment Programme (UNEP), the World Organisation for Animal Health (WOAH, founded as OIE), and the World Health Organization. Accessed 19 April 2025.
Ho, C.S., Wong, C.T.H., Aung, T.T., Lakshminarayanan, R., Mehta, J.S., Rauz, S., McNally, A., Kintses, B., Peacock, S.J., de la Fuente-Nunez, C., Hancock, R.E.W, Ting, D.S.J., 2024. Antimicrobial resistance: a concise update. Lancet Microbe. 2025 Jan;6(1):100947. doi: 10.1016/j.lanmic.2024.07.010. Epub. PMID: 39305919. Accessed 28 May 2025.
Lewnard, J.A., Charani, E., Gleason, A., Hsu, L.Y., Khan, W.A., Karkey, A., Chandler, C.I.R., Mashe, T., Khan, E.A., Bulabula, A.N.H., Donado-Godoy, P., Laxminarayan, R., 2024. Burden of bacterial antimicrobial resistance in low-income and middle-income countries avertible by existing interventions: an evidence review and modelling analysis. Lancet. 403(10442):2439-2454. doi: 10.1016/S0140-6736(24)00862-6. Accessed 19 April 2025.
Murray, C.J.L, et al., 2022. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet 399.10325: 629-655. Accessed 21 February 2025.
Naghavi, M., et al., 2024. Global burden of bacterial antimicrobial resistance 1990–2021: a systematic analysis with forecasts to 2050. The Lancet 404.10459: 1199-1226. Accessed 19 April 2025.
O’Neill, J., 2016. Tackling drug-resistant infections globally: Final report and recommendations. London: HM Government and Wellcome Trust. Review on Antimicrobial Resistance, chaired by Jim O’Neill. Accessed 19 April 2025.
UNEP, no date. Why does AMR matter? United Nations Environment Programme (UNEP). Accessed 19 April 2025.
UNGA, 2024. UN General Assembly Political declaration of the high-level meeting on antimicrobial resistance– resolution A/79/L.5. United Nations General Assembly (UNGA). Accessed 19 April 2025.
WHO, 2015. Global Action Plan on Antimicrobial Resistance. (World Health Organization (WHO). Accessed 19 April 2025.
WHO, 2016. International Health Regulations (2005), 3rd ed. World Health Organization (WHO). Accessed 26 May 2025.
WHO, 2023. Antimicrobial resistance. World Health Organization (WHO). Accessed 27 May 2025.
WHO, 2024. Tuberculosis: Multidrug-resistant (MDR-TB) or rifampicin-resistant TB (RR-TB). World Health Organization (WHO). Accessed 19 April 2025.
WHO, no date. HIV drug resistance. World Health Organization (WHO). Accessed 19 April 2025.
WHO, no date a. One Health. World Health Organization (WHO). Accessed 19 April 2025.
WHO, no date b. Global Antimicrobial Resistance and Use Surveillance System (GLASS). World Health Organization (WHO). Accessed 19 April 2025.
WHO, no date c. Global Antibiotic Research and Development Partnership. World Health Organization (WHO). Accessed 19 April 2025.
WOAH, no date. ANIMUSE (the global database on ANImal antiMicrobial USE), World Organisation for Animal Health (WOAH). Accessed 19 April 2025.