Diarrhoeal Diseases
Diarrhoeal diseases are infectious diseases, contaminants and other causes of diarrhoea. Diarrhoea is defined as the passage of three or more loose or liquid stools per day, or more frequently than is normal for the individual. Diarrhoeal disease is the third leading cause of death in children 1–59 months of age. It is both preventable and treatable. (WHO, 2024a).
Primary reference(s)
WHO, 2024a. Diarrhoea. World Health Organization (WHO).. Accessed 26 March 2025.
Annotations
Additional scientific description
Diarrhoeal disease is the third leading cause of death in children under 5 years old and is responsible for killing around 443,832 children every year. Diarrhoea can last several days and can leave the body without the water and salts that are necessary for survival. In the past, for most people, severe dehydration and fluid loss were the main causes of diarrhoea-associated deaths. Now, other causes such as septic bacterial infections are likely to account for an increasing proportion of all diarrhoea-associated deaths. Children who are malnourished or have impaired immunity, as well as people living with HIV, are most at risk of life-threatening diarrhoea (WHO, 2024).
Diarrhoea is defined as the passage of 3 or more loose or liquid stools per day (or more frequent passage than is normal for the individual). Frequent passing of formed stools is not diarrhoea, nor is the passing of loose, pasty stools by breastfed babies.
Diarrhoea is usually a symptom of an infection in the intestinal tract, which can be caused by a variety of bacterial, viral and parasitic organisms. Infection is spread through contaminated food or drinking water, or from person-to-person as a result of poor hygiene.
Interventions to prevent diarrhoea, including safe drinking water, use of improved sanitation and hand washing with soap, can reduce disease risk. Diarrhoea should be treated with oral rehydration solution (ORS), a solution of clean water, sugar and salt. In addition, a 10-14-day supplemental treatment course of dispersible zinc tablets shortens diarrhoea duration and improves outcomes.
There are 3 clinical types of diarrhoea:
- acute watery diarrhoea - lasts several hours or days and includes cholera
- acute bloody diarrhoea - also called dysentery
- persistent diarrhoea - lasts 14 days or longer.
Metrics and numeric limits
Diarrhoeal disease is a leading cause of child mortality and morbidity in the world and mostly results from contaminated food and water sources. Worldwide, 780 million individuals lack access to improved drinking water and 2.5 billion lack improved sanitation. Diarrhoea due to infection is widespread throughout developing countries (WHO, 2024a).
In low-income countries, children under 3 years old experience on average three episodes of diarrhoea every year. Each episode deprives the child of the nutrition necessary for growth. As a result, diarrhoea is a major cause of malnutrition, and malnourished children are more likely to fall ill from diarrhoea (WHO, 2024a).
Key relevant UN convention / multilateral treaty
International Health Regulations (2005), 3rd ed. (WHO, 2016).
Drivers
Hazard drivers include infection, underlying malnutrition, water contamination and other causes such as poor personal hygiene (WHO, 2024). In summary, these are described below:
- Infection: Diarrhoea is a symptom of infections caused by a host of bacterial, viral and parasitic organisms, most of which are spread by faeces-contaminated water. Infection is more common when there is a shortage of adequate sanitation and hygiene and safe water for drinking, cooking and cleaning. Among children under 5 years of age, the most common viral pathogens are rotavirus, norovirus, adenovirus and astrovirus. Bacterial pathogens include Escherichia coli, Salmonella spp., Shigella spp., and Campylobacter spp., while parasitic pathogens include Cryptosporidium, Giardia, and Entamoeba spp. Rotavirus and E. coli are the most common pathogens among children across all age groups, while parasitic pathogens are prevalent in children aged 3-5 years. Bacterial pathogens, including E. coli, Salmonella, and Shigella, were common in the children aged 6 to 10-year age group, as were rotavirus, norovirus, and sapovirus. Location-specific etiologic patterns also need to be considered (WHO, 2024a).
- Malnutrition: Children who die from diarrhoea often suffer from underlying malnutrition, which makes them more vulnerable to diarrhoea. Each diarrhoeal episode, in turn, makes their malnutrition even worse. Diarrhoea is a leading cause of malnutrition in children under 5 years old (WHO, 2024a).
- Source: Water contaminated with human faeces, for example from sewage, septic tanks and latrines, is of particular concern. Animal faeces also contain microorganisms that can cause diarrhoea (WHO, 2024a).
- Other causes: Diarrhoeal disease can also spread from person-to-person, aggravated by poor personal hygiene. Food is another major cause of diarrhoea when it is prepared or stored in unhygienic conditions. Unsafe domestic water storage and handling is also an important risk factor. Fish and seafood from polluted water may also contribute to the disease (WHO, 2024a).
Impacts
Globally, there are nearly 1.7 billion cases of childhood diarrhoeal disease every year (WHO, 2024a). Diarrhoea is a leading cause of malnutrition in children under 5 years old (WHO, 2024a).
The most severe threat posed by diarrhoea is dehydration. During a diarrhoeal episode, water and electrolytes (sodium, chloride, potassium and bicarbonate) are lost through liquid stools, vomit, sweat, urine and breathing (WHO, 2024a). Dehydration occurs when these losses are not replaced.
WHO (2024a) describes the degree of dehydration as rated on a scale of 3.
- severe dehydration (at least two of the following signs):
- lethargy/unconsciousness
- sunken eyes
- unable to drink or drink poorly
- skin pinch goes back very slowly (≥2 seconds)
- some dehydration (two or more of the following signs):
- restlessness, irritability
- sunken eyes
- drinks eagerly, thirsty
- no dehydration (not enough signs to classify as some or severe dehydration)
Multi-hazard context
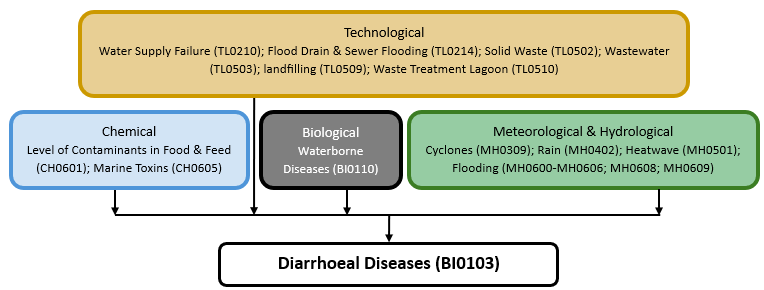
The figure below summarises common interactions between diarrhoeal diseases and other hazards. This information should be used with caution and not be solely relied upon in Disaster Risk Management, particularly as some interactions may not have been included. Note that hazardous events occurring together or locally in space or time may not necessarily cause, amplify, or be otherwise related to each other. Specific examples of multi-hazard context can be found in the ‘Hazard drivers’ and ‘Impacts’ sections above.
Multi-hazard diagram
Risk Management
WHO (2024a) has identified key measures to treat diarrhoea as follows:
- Rehydration with oral rehydration salts (ORS) solution. ORS is a mixture of clean water, salt and sugar. It costs a few cents per treatment. ORS is absorbed in the small intestine and replaces the water and electrolytes lost in the faeces.
- Zinc supplements reduce the duration of a diarrhoea episode by 25% and are associated with a 30% reduction in stool volume.
- Rehydration with intravenous fluids in case of severe dehydration or shock.
- Nutrient-rich foods. The vicious circle of malnutrition and diarrhoea can be broken by continuing to give nutrient-rich foods – including breast milk – during an episode, and by giving a nutritious diet – including exclusive breastfeeding for the first 6 months of life – to children when they are well.
Consulting a health professional, in particular for the management of persistent diarrhoea, when there is blood in the stool, or if there are signs of dehydration, is recommended (WHO, 2024a).
WHO (2024a) recommends the following key measures to prevent diarrhoea to include:
- access to safe drinking water
- use of improved sanitation
- hand washing with soap
- exclusive breastfeeding for the first 6 months of life
- good personal and food hygiene
- health education about how infections spread
- rotavirus vaccination.
In addition, WHO works with Member States and other partners to:
- promote national policies and investments that support case management of diarrhoea and its complications as well as increasing access to safe drinking water and sanitation in developing countries;
- conduct research to develop and test new diarrhoea prevention and control strategies in this area;
- build capacity in implementing preventive interventions, including sanitation, source water improvements, and household water treatment and safe storage;
- develop new health interventions, such as the rotavirus immunization; and
- help to train health workers, especially at the community level (WHO, 2024a).
Monitoring
WHO supports countries to conduct all-hazards strategic risk assessment in the contexts of health emergencies and disasters, which results in the development of a country risk profile. Empowered with the country risk profile, inclusive of a seasonal risk calendar, countries can anticipate potential emergencies before they occur to trigger early alerts and inform early actions (WHO, 2021).
Many individual diarrhoeal diseases have monitoring systems, For example, cholera surveillance should be part of an integrated disease surveillance system. This includes timely reporting, data analysis, interpretation and sharing of information from local to global levels. Rapid diagnostic tests (RDTs) are useful for early detection of probable cholera outbreaks, but confirmation requires laboratory testing by culture, seroagglutination or polymerase chain reaction (PCR) (WHO, 2024b). Countries at risk or affected by cholera should strengthen their surveillance systems according to the revised Global Taskforce on Cholera Control (GTFCC) recommendations to quickly detect and respond to outbreaks (GTFCC, 2025).
WHO's Early Warning, Alert and Response System (EWARS) has been designed to improve disease outbreak detection in emergency settings, such as in countries in conflict or following a natural disaster. It is a simple and cost-effective way to rapidly set up a disease surveillance system. EWARS is deployed during an emergency as an adjunct to the national disease surveillance system. WHO works with Ministries of Health and health sector partners to train local health workers to use the system. After the emergency, EWARS should re-integrate back into the national system (WHO, no date).
References
GTFCC, 2024. Public health surveillance for cholera-guidance document 2024. The Global Task Force on Cholera Control. Accessed 26 March 2025.
WHO no date. Early Warning, Alert and Response System (EWARS). World Health Organization (WHO). Accessed 26 March 2025.
WHO, 2016. International Health Regulations (2005), 3rd ed. World Health Organization (WHO). Accessed 26 March 2025.
WHO, 2021. Strategic toolkit for assessing risks (STAR): a comprehensive toolkit for all-hazards health emergency risk assessment. World Health Organization (WHO). Accessed 13 February 2025.
WHO, 2024a. Diarrhoeal disease. World Health Organization (WHO). Accessed 26 March 2025.
WHO, 2024b. Cholera. World Health Organization (WHO). Accessed 26 March 2025.